Each radiopaque implant contains 68 mg of etonogestrel; the release rate is approximately 60-70 μg/day in week 5-6 and has decreased to approximately 35-45 μg/day at the end of the first year, to approximately 30-40 μg/day at the end of the second year and to approximately 25-30 μg/day at the end of the third year. The innovative applicator is designed to be operated with one hand and to help facilitate correct subdermal insertion of the implant.
Implanon NXT is a radiopaque, non-biodegradable, progestagen-only, flexible implant preloaded in a sterile, ready-for-use, disposable applicator.
Excipients/Inactive Ingredients: Core: Ethylene vinyl acetate copolymer (28% vinyl acetate, 43 mg) barium sulfate (15 mg), magnesium stearate (0.1 mg).
Skin: Ethylene vinyl acetate copolymer (15% vinyl acetate, 15 mg).
Pharmacotherapeutic group: progestagens. ATC-classification: G03AC08.
Pharmacology: Pharmacodynamics: The Implanon NXT implant is a non-biodegradable, radiopaque, etonogestrel-containing implant for subdermal use, preloaded in a sterile, innovative, disposable applicator. Etonogestrel is the biologically active metabolite of desogestrel, a progestagen widely used in OCs. It is structurally derived from 19-nortestosterone and binds with high affinity to progesterone receptors in the target organs. The contraceptive effect of etonogestrel is primarily achieved by inhibition of ovulation. Ovulations were not observed in the first two years of use of the implant and only rarely in the third year. Besides inhibition of ovulation, etonogestrel also causes changes in the cervical mucus, which hinders the passage of spermatozoa. Clinical trials were conducted in women between 18 and 40 years. Although no direct comparison was made, the contraceptive efficacy appeared to be at least comparable to that known for combined OCs (over 99%). The high degree of protection against pregnancy is obtained, amongst other reasons, because the contraceptive action of Implanon NXT is not dependent on adherence to a daily, weekly, or monthly dosing regimen by the woman herself. The contraceptive action of etonogestrel is reversible, which is apparent from the rapid return of the normal menstrual cycle after removal of the implant. Although etonogestrel inhibits ovulation, ovarian activity is not completely suppressed. Mean estradiol concentrations remain above the level seen in the early-follicular phase. In a two-year study, in which the bone mineral density in 44 users has been compared with that in a control group of 29 IUD-users no adverse effects on bone mass have been observed. No clinically relevant effects on lipid metabolism have been observed. The use of progestagen-containing contraceptives may have an effect on insulin resistance and glucose tolerance. Clinical trials further indicate that users of Implanon NXT often have a less painful menstrual bleeding (dysmenorrhea).
Implant insertion and removal characteristics: In a clinical trial, Implanon NXT was inserted in 301 women. The mean insertion time (from the removal of the protection cap of the applicator until retraction of the needle from the arm) was 27.9 seconds (standard deviation (SD)=29.3, n=291). After insertion, 300 out of 301 (99.7%) Implanon NXT implants were palpable. The single, non-palpable implant was not inserted according to the instructions. For 293 of the 301 subjects, data on palpability was gathered before removal. The implant was palpable for all 293 subjects with data on palpability. For four subjects, palpability was not assessed and another four subjects were lost to follow-up before removal.
In two clinical trials with Implanon NXT implants, a total of 116 subjects underwent two-dimensional x-ray assessments at (after) insertion and/or (before) removal. For 101 out of 103 (98.1%) subjects for whom x-ray assessments were performed at insertion and before removal, Implanon NXT implants were clearly visible; for two subjects the implants were not clearly visible after insertion but were clearly visible before removal. The implants of the 13 subjects with x-ray assessment only at insertion (n=12) or only before removal (n=1) were all clearly visible.
Pharmacokinetics: Absorption: After the insertion of the implant, etonogestrel is rapidly absorbed into the circulation. Ovulation-inhibiting concentrations are reached within 1 day. Maximum serum concentrations (between 472 and 1270 pg/ml) are reached within 1 to 13 days. The release rate of the implant decreases with time. As a result serum concentrations decline rapidly over the first few months. By the end of the first year a mean concentration of approximately 200 pg/ml (range 150-261 pg/ml) is measured, which slowly decreases to 156 pg/ml (range 111-202 pg/ml) by the end of the third year. The variations observed in serum concentrations can be partly attributed to differences in body weight.
Distribution: Etonogestrel is for 95.5-99% bound to serum proteins, predominantly to albumin and to a lesser extent to sex hormone binding globulin. The central and total volume of distribution are 27 l and 220 l, respectively, and hardly change during the use of Implanon NXT.
Metabolism: Etonogestrel undergoes hydroxylation and reduction. Metabolites are conjugated to sulfates and glucuronides. Animal studies show that enterohepatic circulation probably does not contribute to the progestagenic activity of etonogestrel.
Elimination: After intravenous administration of etonogestrel, the mean elimination half-life is approximately 25 hours and the serum clearance is approximately 7.5 l/hour. Both clearance and elimination-half-life remain constant during the treatment period. The excretion of etonogestrel and its metabolites, either as free steroids or as conjugates, is with urine and feces (ratio 1.5:1). After insertion in lactating women, etonogestrel is excreted in breast milk with a milk/serum ratio of 0.44-0.50 during the first four months. In lactating women, the mean transfer of etonogestrel to the infant is approximately 0.2% of the estimated absolute maternal etonogestrel daily dose (2.2% when values are normalized per kg body weight). Concentrations show a gradual and statistically significant decrease over the time.
Toxicology: Preclinical safety data: Toxicological studies did not reveal any effects other than those, which can be explained on the basis of the hormonal properties of etonogestrel, regardless of the route of administration.
Pregnancy should be excluded before insertion of Implanon NXT.
Healthcare professionals (HCPs) are strongly recommended to participate in a training session to become familiar with the use of the Implanon NXT applicator and the techniques for insertion and removal of the Implanon NXT implant and where appropriate, request supervision prior to inserting or removing the implant.
Before inserting the implant, carefully read and follow the instructions for insertion and removal of the implant in "How to insert Implanon NXT" and "How to remove Implanon NXT" as follows.
If patient is unsure of the necessary steps to safely insert and/or remove Implanon NXT, do not attempt the procedure.
How to use Implanon NXT: Implanon NXT is a long-acting hormonal contraceptive. A single implant is inserted subdermally and can left in place for three years. Remove the implant no later than three years after the date of insertion. The user should be informed that she can request the removal of Implant at any time. HCPs may consider earlier replacement of the implant in heavier women (see Warnings under Precautions). After the removal of the implant, immediate insertion of another implant will result in continued contraceptive protection. If the woman does not wish to continue using Implanon NXT, but wants to continue preventing pregnancy, another contraceptive method should be recommended.
The basis for successful use and subsequent removal of the Implanon NXT implant is a correct and carefully performed subdermal insertion of the implant in accordance with the instructions.
If the implant is not inserted in accordance with the instructions (see
"How to insert Implanon NXT"), and on the correct day (see "When to insert Implanon NXT"), this may result in an unintended
pregnancy. An implant inserted more deeply than subdermally (deep insertion) may not be palpable and the localization and/or removal can be difficult (see "How to remove Implanon NXT" as follows and Warnings under Precautions).
The Implanon NXT implant should be inserted subdermally just under the skin at the inner side of the non-dominant upper arm. The insertion site is overlying the triceps muscle about 8-10 cm (3-4 inches) from the medial epicondyle of the humerus and 3-5 cm (1.25-2 inches) posterior to (below) the sulcus (groove) between the biceps and triceps muscles. This location is intended to avoid the large blood vessels and nerves lying within and surrounding the sulcus.
Immediately after insertion, the presence of the implant should be verified by palpation. In case the implant cannot be palpated or when the presence of the implant is doubtful, see 'How to insert Implanon NXT' as follows.
The Implanon NXT package contains a User Card intended for the woman which records the batch number of the implant. HCPs are requested to record the date of insertion, the arm of insertion, and the intended day of removal on the User Card. The package also includes adhesive label intended for HCP records showing the batch number.
When to insert Implanon NXT: IMPORTANT: Rule out pregnancy before inserting the implant.
Timing of insertion depends on the woman's recent contraceptive history, as follows: No preceding hormonal contraceptive use in the past months: The implant should be inserted between Day 1 (first day of menstrual bleeding) and Day 5 of the menstrual cycle, even if the woman is still bleeding.
If inserted as recommended, back-up contraception is not necessary. If deviating from the recommended timing of insertion, the woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded.
Switching contraceptive method to Implanon NXT: Changing from a combined hormonal contraceptive method (combined oral contraceptive (COC), vaginal ring, or transdermal patch): The implant should be inserted preferably on the day after the last active tablet (the last tablet containing the active substances) of the previous COC, but at the latest on the day following the usual tablet-free or placebo tablet interval of the previous COC. In case a vaginal ring or transdermal patch has been used, the implant should be inserted preferably on the day of removal, but at the latest when the next application would have been due.
If inserted as recommended, back-up contraception is not necessary. If deviating from the recommended timing of insertion, the woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded.
Changing from a progestagen-only contraceptive method (e.g. progestagen-only pill, injectable, implant, or intrauterine system [IUS]): As there are several types of progestagen-only methods, the insertion of the implant must be performed as follows: Injectable contraceptives: Insert the implant on the day the next injection is due.
Progestagen-only pill: A woman may switch from the progestagen-only pill to Implanon NXT on any day of the month. The implant should be inserted within 24 hours after taking the tablet.
Implant/Intrauterine system (IUS): Insert the implant on the same day the previous implant or IUS is removed.
If inserted as recommended, back-up contraception is not necessary. If deviating from the recommended timing of insertion, the woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded.
Following abortion or miscarriage: First trimester: The implant should be inserted within 5 days following a first trimester abortion or miscarriage.
Second trimester: Insert the implant between 21 to 28 days following second trimester abortion or miscarriage.
If inserted as recommended, back-up contraception is not necessary. If deviating from the recommended timing of insertion, the woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded.
Postpartum: Breast-feeding: The implant should be inserted after the fourth postpartum week (see Use in Pregnancy & Lactation). The woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded.
Not breast-feeding: The implant should be inserted between 21 to 28 days postpartum. If inserted as recommended, back-up contraception is not necessary. If the implant is inserted later than 28 days postpartum, the woman should be advised to use a barrier method until 7 days after insertion. If intercourse has already occurred, pregnancy should be excluded.
How to insert Implanon NXT: The basis for successful use and subsequent removal of Implanon NXT is a correct and carefully performed subdermal insertion of the implant in the non-dominant arm in accordance with the instructions. Both the HCP and the woman should be able to feel the implant under the woman's skin after placement.
The implant should be inserted subdermally just under the skin at the inner side of the non-dominant upper arm.
An implant inserted more deeply than subdermally (deep insertion) may not be palpable and the localization and/or removal can be difficult (see "How to remove Implanon NXT" as follows and Warnings under Precautions).
If the implant is inserted deeply, neural or vascular damage may occur. Deep or incorrect insertions have been associated with paresthesia (due to neural damage) and migration of the implant (due to intramuscular or fascial insertion), and in rare cases with intravascular insertion.
Insertion of Implanon NXT should be performed under aseptic conditions and only by a qualified HCP who is familiar with the procedure. Insertion of the implant should only be performed with the preloaded applicator.
Insertion Procedure: To help make sure the implant is inserted just under the skin, the HCP should be positioned to see the advancement of the needle by viewing the applicator from the side and not from above the arm. From the side view, the insertion site and the movement of the needle just under the skin can be clearly visualized.
Have the woman lie on her back on the examination table with her non-dominant arm flexed at the elbow and externally rotated so that her hand is underneath her head (or as close as possible).
Identify the insertion site, which is at the inner side of the non-dominant upper arm. The insertion site is overlying the triceps muscle about 8-10 cm (3-4 inches) from the medial epicondyle of the humerus and 3-5 cm (1.25-2 inches) posterior to (below) the sulcus (groove) between the biceps and triceps muscles. This location is intended to avoid the large blood vessels and nerves lying within and surrounding the sulcus. If it is not possible to insert the implant in this location (e.g., in women with thin arms), it should be inserted as far posterior from the sulcus as possible.
Make two marks with a surgical marker: first, mark the spot where the implant will be inserted, and second, mark a spot at 5 centimeters (2 inches) proximal (toward the shoulder) to the first mark. This second mark (guiding mark) will later serve as a direction guide during insertion.
After marking the arm, confirm the site is in the correct location on the inner side of the arm.
Clean the skin from the insertion site to the guiding mark with an antiseptic solution.
Anesthetize the insertion area (for example, with anesthetic spray or by injecting 2 ml of 1% lidocaine just under the skin along the planned insertion tunnel).
Remove the sterile preloaded disposable Implanon NXT applicator carrying the implant from its blister. Visually inspect for breaches of packaging integrity prior to use for damages (e.g. torn, punctured, etc). If the packaging has any visual damage that could compromise sterility, do not use the applicator.
Hold the applicator just above the needle at the textured surface area. Remove the transparent protection cap by sliding it horizontally in the direction of the arrow away from the needle. If the cap does not come off easily the applicator should not be used. The HCP should see the white colored implant by looking into the tip of the needle. Do not touch the purple slider until they have fully inserted the needle subdermally, as doing so will retract the needle and prematurely release the implant from the applicator.
If the purple slider is released prematurely, restart the procedure with a new applicator.
With the free hand, stretch the skin around the insertion site towards the elbow.
The implant should be inserted subdermally just under the skin (see Warnings under Precautions).
To help make sure the implant is inserted just under the skin, the HCP should position themselves to see the advancement of the needle by viewing the applicator from the side and not from above the arm. From the side view they can clearly see the insertion site and the movement of the needle just under the skin.
Puncture the skin with the tip of the needle slightly angled less than 30°.
Insert the needle until the bevel (slanted opening of the tip) is just under the skin (and no further). If the HCP inserted the needle deeper than the bevel, withdraw the needle until only the bevel is beneath the skin.
Lower the applicator to a nearly horizontal position. To facilitate subdermal placement, lift the skin with the needle while sliding the needle to its full length. They may feel slight resistance but do not exert excessive force. If the needle is not inserted to its full length, the implant will not be inserted properly.
If the needle tip emerges from the skin before needle insertion is complete, the needle should be pulled back and be readjusted to subdermal position before completing the insertion procedure.
Keep the applicator in the same position with the needle inserted to its full length. If needed, free hand may be used to stabilize the applicator.
Unlock the purple slider by pushing it slightly down. Move the slider fully back until it stops. Do not move the applicator while moving the purple slider. The implant is now in its final subdermal position and the needle is locked inside the body of the applicator. The applicator can now be removed.
If the applicator is not kept in the same position during this procedure or if the purple slider is not moved fully back until it stops, the implant will not be inserted properly and may protrude from the insertion site.
If the implant is protruding from the insertion site, remove the implant and perform a new procedure at the same insertion site using a new applicator.
Do not push the protruding implant back into the incision.
Apply a small adhesive bandage over the adhesion site.
Always verify the presence of the implant in the woman's arm immediately after insertion by palpation. By palpating both ends of the implant, the HCP should be able to confirm the presence of the 4 cm rod. See "If the rod is not palpable after insertion" as follows.
Request that the woman palpate the implant.
Apply sterile gauze with a pressure bandage to minimize bruising. The woman may remove the pressure bandage in 24 hours and the small adhesive bandage over the insertion site after 3-5 days.
Complete the User Card and give it to the woman to keep. Also, complete the adhesive labels and affix it to the woman's medical record.
The applicator is for single use only and must be adequately disposed of, in accordance with local regulations for the handling of biohazardous waste.
If the rod is not palpable after insertion: If the HCP cannot palpate the implant or is in doubt of its presence, the implant may not have been inserted or it may have been inserted deeply: Check the applicator. The needle should be fully retracted and only the purple tip of the obturator should be visible.
Use other methods to confirm the presence of the implant. Given the radiopaque nature of the implant, suitable methods for localization are two-dimensional X-ray and X-ray computerized tomography (CT scan). Ultrasound scanning (USS) with a high-frequency linear array transducer (10 MHz or greater) or magnetic resonance imaging (MRI) may be used. In case these imaging methods fail, it is advised to verify the presence of the implant by measuring the etonogestrel level in a blood sample from the woman. In this case the local Organon office [Organon DPOC +603-2386 2008] will provide the appropriate protocol.
Until the HCP has verified the presence of the implant, the woman must use a non-hormonal contraceptive method.
Deeply-placed implants should be localized and removed as soon as possible to avoid the potential for distant migration (see Warnings under Precautions).
How to remove Implanon NXT: Removal of the implant should only be performed under aseptic conditions by a HCP who is familiar with the removal technique. If unfamiliar with the removal technique, contact the local Organon office [Organon DPOC +603-2386 2008] for further information.
Before initiating the removal procedure, the HCP should assess the location of the implant. Verify the exact location of the implant in the arm by palpation.
If the implant is not palpable, consult the User Card or medical record to verify the arm which contains the implant. If the implant cannot be palpated, it may be deeply located or have migrated. Consider that it may lie close to vessels and nerves. Removal of non-palpable implants should only be performed by a HCP experienced in removing deeply placed implants and familiar with localizing the implant and the anatomy of the arm. Contact the local Organon office [Organon DPOC +603-2386 2008] for further information.
See "Localization and removal of a non-palpable implant" as follows if the implant cannot be palpated.
Procedure for removal of an implant that is palpable: Have the woman lie on her back on the table. The arm should be positioned with the elbow flexed and the hand underneath the head (or as close as possible).
Locate the implant by palpation. Push down the end of the implant closest to the shoulder to stabilize it; a bulge should appear indicating the tip of the implant that is closest to the elbow. If the tip does not pop up, removal of the implant may be more challenging and should be performed by providers experienced with removing deeper implants. Contact the local Organon office [Organon DPOC +603-2386 2008] for further information.
Mark the distal end (end closest to the elbow), for example, with a surgical marker.
Clean the site with an antiseptic solution.
Anesthetize the site, for example, with 0.5 to 1 ml 1% lidocaine where the incision will be made. Be sure to inject the local anesthetic under the implant to keep the implant close to the skin surface. Injection of local anesthetic over the implant can make removal more difficult.
Push down the end of the implant closest to the shoulder to stabilize it throughout the procedure. Starting over the tip of the implant closest to the elbow, make a longitudinal (parallel to the implant) incision of 2 mm towards the elbow. Take care not to cut the tip of the implant.
The tip of the implant should pop out of the incision. If it does not, gently push the implant towards the incision until the tip is visible. Grasp the implant with forceps and if possible, remove the implant. If needed, gently remove adherent tissue from the tip of the implant using blunt dissection. If the implant tip is not exposed following blunt dissection, make an incision into the tissue sheath and then remove the implant with the forceps.
If the tip of the implant does not become visible in the incision, insert forceps (preferably curved mosquito forceps, with the tips pointed up) superficially into the incision. Gently grasp the implant and then flip the forceps over into the other hand. With a second pair of forceps carefully dissect the tissue around the implant and grasp the implant. The implant can then be removed. If the implant cannot be grasped, stop the procedure and refer the woman to a HCP experienced with complex removals or contact the local Organon office [Organon DPOC +603-2386 2008].
Confirm that the entire implant, which is 4 cm long, has been removed by measuring its length. There have been reports of broken implants while in the patient's arm. In some cases, difficult removal of the broken implant has been reported. If a partial implant (less than 4 cm) is removed, the remaining piece should be removed by following the instructions in "How to remove Implanon NXT" previously mentioned.
If the woman would like to continue using Implanon NXT, a new implant may be inserted immediately after the old implant is removed using the same incision as long as the site is in the correct location ("How to replace Implanon NXT" as follows).
After removing the implant, close the incision with a sterile adhesive wound closure.
Apply sterile gauze with a pressure bandage to minimize bruising. The woman may remove the pressure bandage after 24 hours and the sterile adhesive wound closure after 3-5 days.
Localization and removal of a non-palpable implant: There have been occasional reports of migration of the implant; usually this involves minor movement relative to the original position (see also Warnings under Precautions) but may lead to the implant not being palpable at the location in which it was placed. An implant that has been deeply inserted or has migrated may not be palpable and therefore imaging procedures, as described as follows, may be required for localization.
A non-palpable implant should always be located prior to attempting removal. Given the radiopaque nature of the implant, suitable methods for localization include two-dimensional X-ray and X-ray computer tomography (CT). Ultrasound scanning (USS) with a high-frequency linear array transducer (10 MHZ or greater) or magnetic resonance imaging (MRI) may be used. Once the implant has been localized in the arm, the implant should be removed by a HCP experienced in removing deeply placed implants and familiar with the anatomy of the arm. The use of ultrasound guidance during the removal should be considered.
If the implant cannot be found in the arm after comprehensive localization attempts, consider applying imaging techniques to the chest as rare events of migration to the pulmonary vasculature have been reported. If the implant is located in the chest, surgical or endovascular procedures may be needed for removal; HCPs familiar with the anatomy of the chest should be consulted.
If at any time these imaging methods fail to locate the implant, etonogestrel blood level determination can be used for verification of the presence of the implant. Please contact the local Organon office [Organon DPOC +603-2386 2008] for further guidance.
If the implant migrates within the arm, removal may require a minor surgical procedure with a larger incision or a surgical procedure in an operating room. Removal of deeply inserted implants should be conducted with caution in order to help prevent damage to deeper neural or vascular structures in the arm. Non-palpable and deeply inserted implants should be removed by HCPs familiar with the anatomy of the arm and removal of deeply inserted implants.
Exploratory surgery without knowledge of the exact location of the implant is strongly discouraged.
Please contact the local Organon office [Organon DPOC +603-2386 2008] for further guidance.
How to replace Implanon NXT: Immediate replacement can be done after removal of the previous implant and is similar to the insertion procedure previously described in "How to insert Implanon NXT".
The new implant may be inserted in the same arm, and through the same incision from which the previous implant was removed, as long as the site is in the correct location i.e., 8-10 cm from the medial epicondyle of the humerus and 3-5 cm posterior to (below) the sulcus (see "How to insert Implanon NXT" previously). If the same incision is being used to insert a new implant, anesthetize the insertion site (e.g. 2 ml lidocaine (1%)) applied just under the skin commencing at the removal incision along the 'insertion canal' and follow the subsequent steps in the insertion instructions.
An implant should always be removed before inserting a new one. There are no data available on overdose with etonogestrel. There have been no reports of serious deleterious effects from an overdose of contraceptives in general.
Progestagen-only contraceptives should not be used in the presence of any of the conditions listed as follows. Should any of the conditions appear for the first time during the use of Implanon NXT, the product should be stopped immediately.
Known or suspected pregnancy; Active venous thromboembolic disorder; Known or suspected sex steroid sensitive malignancies; Presence or history of liver tumours (benign or malignant); Presence or history of severe hepatic disease as long as liver function values have not returned to normal; Undiagnosed vaginal bleeding; Hypersensitivity to the active substance or to any of the excipients of Implanon NXT.
Warnings: If any of the conditions/risk factors mentioned as follows is present, the benefits of progestagen use should be weighed against the possible risks for each individual woman and discussed with the woman before she decides to start with Implanon NXT. In the event of aggravation, exacerbation or first appearance of any of these conditions, the woman should contact her HCP. The HCP should then decide on whether the use of Implanon NXT should be discontinued.
Carcinoma of the Breast: The risk for breast cancer increases in general with increasing age. During the use of (combined) oral contraceptives (OCs) the risk of having breast cancer diagnosed is slightly increased. This increased risk disappears gradually within 10 years after discontinuation of OC use and is not related to the duration of use, but to the age of the woman when using the OC. The expected number of cases diagnosed per 10 000 women who use combined OCs (up to 10 years after stopping) relative to never users over the same period have been calculated for the respective age groups to be: 4.5/4 (16-19 years), 17.5/16 (20-24 years), 48.7/44 (25-29 years), 110/100 (30-34 years), 180/160 (35-39 years) and 260/230 (40-44 years). The risk in users of contraceptive methods, which only contain progestagens, is possibly of similar magnitude as that associated with combined OCs. However, for these methods, the evidence is less conclusive. Compared to the risk of getting breast cancer ever in life, the increased risk associated with OCs is low. The cases of breast cancer diagnosed in OC users tend to be less advanced than in those who have not used OCs. The increased risk observed in OC users may be due to an earlier diagnosis, biological effects of the OC or a combination of both.
Liver Disease: When acute or chronic disturbances of liver function occur the woman should be referred to a specialist for examination and advice.
Thrombotic and Other Vascular Events: Epidemiological investigations have associated the use of combined OCs with an increased incidence of venous thromboembolism (VTE, deep venous thrombosis and pulmonary embolism). Although the clinical relevance of this finding for etonogestrel (the biologically active metabolite of desogestrel) used as a contraceptive in the absence of an estrogenic component is unknown, the implant should be removed in the event of a confirmed thrombosis. Removal of the implant should also be considered in case of long-term immobilization due to surgery or illness. Although Implanon NXT is a progestagen-only contraceptive, it is recommended to assess risk factors which are known to increase the risk of venous and arterial thromboembolism. Women with a history of thromboembolic disorders should be made aware of the possibility of a recurrence.
There have been postmarketing reports of serious arterial and venous thromboembolic events, including cases of pulmonary emboli (some fatal), deep vein thrombosis, myocardial infarction, and strokes, in women using etonogestrel implants. Implanon NXT should be removed in the event of a thrombosis.
Elevated Blood Pressure: If a sustained hypertension develops during the use of Implanon NXT, or if a significant increase in blood pressure does not adequately respond to antihypertensive therapy, Implanon NXT should be removed.
Carbohydrate and Lipid Metabolic Effects: Although progestagens may have an effect on peripheral insulin resistance and glucose tolerance, there is no evidence for a need to alter the therapeutic regimen in diabetics using progestagen-only contraceptives. However, diabetic women should be carefully observed while using progestagen-only contraceptives.
Women who are being treated for hyperlipidemia should be followed closely if they elect to use Implanon NXT. Some progestagens may elevate LDL levels and may render the control of hyperlipidemia more difficult.
Chloasma: Chloasma may occasionally occur, especially in women with a history of chloasma gravidarum. Women with a tendency to chloasma should avoid exposure to the sun or ultraviolet radiation whilst using Implanon NXT.
Body Weight: The contraceptive effect of Implanon NXT is related to the plasma levels of etonogestrel, which are inversely related to body weight, and decrease with time after insertion. The clinical experience in heavier women in the third year of use is limited. Therefore it cannot be excluded that the contraceptive effect in these women during the third year of use may be lower than for women of normal weight. HCPs may therefore consider earlier replacement of the implant in heavier women.
Complications of Insertion: Expulsion may occur especially if the implant is inserted not according to the instructions given in How to insert Implanon NXT under Dosage & Administration, or as a consequence of a local inflammation.
There have been reports of migration of the implant within the arm from the insertion site, which may be related to a deep insertion (see also How to insert Implanon NXT under Dosage & Administration), or external forces (e.g. manipulation of the implant or contact sports). There also have been rare postmarketing reports of implants located within the vessels of the arm and the pulmonary artery, which may be related to deep insertions or intravascular insertion. In cases where the implant has migrated within the arm from the insertion site, localization may be more difficult and removal may require a minor surgical procedure with a larger incision or a surgical procedure in an operating room. In cases where the implant has migrated to the pulmonary artery, endovascular or surgical procedures may be needed for removal (see also How to remove Implanon NXT under Dosage & Administration). If at any time the implant cannot be palpated, it should be localized and removal is recommended. If the implant is not removed, contraception and the risk of progestagen-related undesirable effects may continue beyond the time desired by the woman.
Ovarian Cysts: With all low-dose hormonal contraceptives, follicular development may occur and occasionally the follicle may continue to grow beyond the size it would attain in a normal cycle. Generally, these enlarged follicles disappear spontaneously. Often, they are asymptomatic; in some cases they are associated with mild abdominal pain. They rarely require surgical intervention.
Ectopic Pregnacies: The protection with traditional progestagen-only contraceptives against ectopic pregnancies is not as good as with combined OCs, which has been associated with the frequent occurrence of ovulations during the use of these methods. Despite the fact that Implanon NXT will consistently inhibits ovulation, ectopic pregnancy should be taken into account in the differential diagnosis if the woman gets amenorrhea or abdominal pain.
Other Conditions: The following conditions have been reported both during pregnancy and during sex steroid use, but an association with the use of progestagens has not been established: jaundice and/or pruritus related to cholestasis; gallstone formation; porphyria; systemic lupus erythematosus; hemolytic uraemic syndrome; Sydenham's chorea; herpes gestationis; otosclerosis-related hearing loss and (hereditary) angioedema.
Medical examination/consultation: Prior to the initiation or reinstitution of Implanon NXT a complete medical history (including family medical history) should be taken and pregnancy should be excluded. Blood pressure should be measured and a physical examination should be performed, guided by the contraindications (see Contraindications) and warnings (see previously mentioned Warnings). It is recommended that the woman returns for a medical check-up three months after insertion of Implanon NXT. During this check-up, the blood pressure should be measured and an enquiry should be made after any questions, complaints or the occurrence of undesirable effects. The frequency and nature of further periodic checks should be adapted to the individual woman, guided by clinical judgement.
Women should be advised that Implanon NXT does not protect against HIV (AIDS) and other sexually transmitted diseases.
Reduced efficacy with concomitant medications: The efficacy of Implanon NXT may be reduced when concomitant medications that decrease the plasma concentration of etonogestrel are used (see Interactions).
Changes in the menstrual bleeding pattern: During the use of Implanon NXT, women are likely to have changes in their menstrual bleeding pattern. These may include changes in bleeding frequency (absent, less, more frequent or continuous), intensity (reduced or increased) or duration. Amenorrhea was reported in about 1 of 5 women while another 1 of 5 women reported frequent and/or prolonged bleeding. Dysmenorrhea tended to improve while using Implanon NXT. The bleeding pattern experienced during the first three months is broadly predictive of future bleeding patterns for many women. Information, counseling and the use of a bleeding diary can improve the woman's acceptance of a bleeding pattern. Evaluation of vaginal bleeding should be done on an ad hoc basis and may include an examination to exclude gynecological pathology or pregnancy.
Broken or bent implant: There have been reports of broken or bent implants, which may be related to external forces (e.g. manipulation of the implant or contact sports) while in the patient's arm. There have also been reports of migration of a broken implant fragment within the arm. Based on in vitro data, when the implant is broken or bent, the release rate of etonogestrel may be slightly increased. This change is not expected to have clinically meaningful effects.
When an implant is removed, it is important to remove it in its entirety (see How to remove Implanon NXT under Dosage & Administration).
Effects on ability to drive and use machines: No observed effects.
Implanon NXT is not indicated during pregnancy. If pregnancy occurs during use of Implanon NXT, the implant should be removed. Animal studies have shown that very high doses of progestagenic substances may cause masculinisation of female fetuses. Extensive epidemiological studies have revealed neither an increased risk of birth defects in children born to women who used OCs prior to pregnancy, nor of a teratogenic effect when OCs were inadvertently used during pregnancy. Although this probably applies to all OCs, it is not clear whether this is also the case for Implanon NXT.
Pharmacovigilance data with various etonogestrel- and desogestrel-containing products (etonogestrel is a metabolite of desogestrel) do not indicate an increased risk.
Clinical data indicate that Implanon NXT does not influence the production or the quality (protein, lactose or fat concentrations) of breast milk. However, small amounts of etonogestrel are excreted in breast milk. Based on an average daily milk ingestion of 150 ml/kg, the mean daily infant etonogestrel dose calculated after one month of etonogestrel release is approximately 27 ng/kg/day. This corresponds to approximately 2.2% of the weight-adjusted maternal daily dose and to approximately 0.2% of the estimated absolute maternal daily dose. Subsequently the milk etonogestrel concentration decreases with time during the lactation period.
Long-term data are available on 38 children, whose mothers had an implant inserted during the 4th to 8th week postpartum. They were breast-fed for a mean duration of 14 months and followed-up to 36 months of age. Evaluation of growth, and physical and psychomotor development did not indicate any differences in comparison to nursing infants whose mothers used an IUD (n=33). Nevertheless, development and growth of the child should be carefully followed. Based on the available data, Implanon NXT may be used during lactation and should be inserted after the 4th post partum week.
Serious undesirable effects: See Warnings under Precautions.
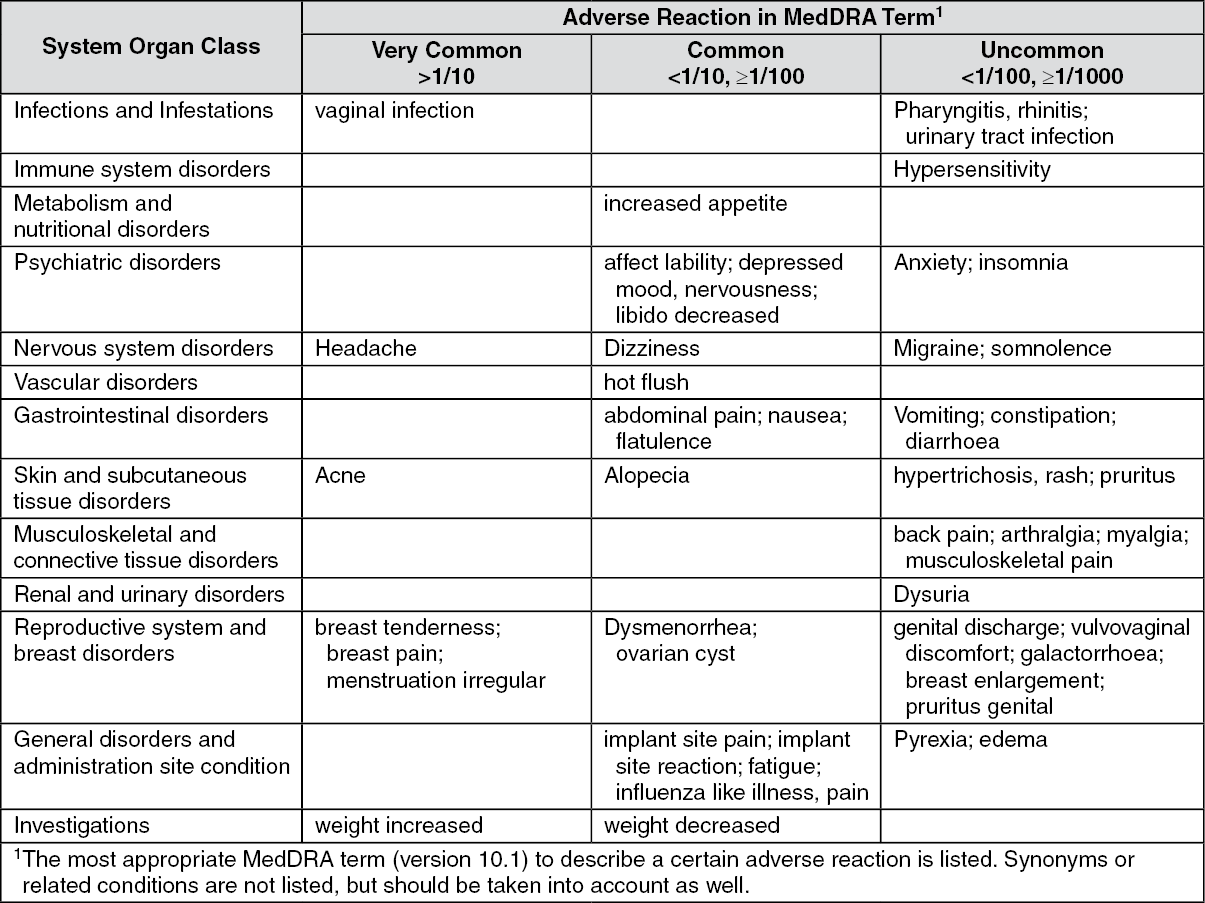
Other possible undesirable effects: During the use of Implanon NXT, women are likely to have changes in their menstrual bleeding pattern. These may include changes in bleeding frequency (absent, less, more frequent or continuous), intensity (reduced or increased) or duration. Amenorrhea was reported in about 1 of 5 women while another 1 of 5 women reported frequent and/or prolonged bleeding. Occasionally, heavy bleeding has been reported. In clinical trials, bleeding changes were the most common reason for stopping treatment (about 11%). Dysmenorrhea tended to improve while using Implanon NXT. The bleeding pattern experienced during the first three months is broadly predictive of future bleeding patterns for many women.
Possibly related undesirable effects reported in clinical trials have been listed in the table as follows. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In a clinical trial of Implanon NXT, in which investigators were asked to examine the implant site after insertion, implant site reactions were reported in 8.6% of women. Erythema was the most frequent implant site complication, reported during and/or shortly after insertion, occurring in 3.3% of subjects. Additionally, hematoma (3.0%), bruising (2.0%), pain (1.0%), and swelling (0.7%) were reported.
During post marketing surveillance, a clinically relevant rise in blood pressure has been observed in rare cases. Seborrhea has also been reported. Anaphylactic reactions, urticaria, angioedema, aggravation of angioedema and/or aggravation of hereditary angioedema may occur.
Insertion or removal of the implant may cause some vasovagal reactions (for example: hypotension, dizziness, or syncope), bruising, slight local irritation, pain or itching. Fibrosis at the implant site may occur, a scar may be formed or an abscess may develop. Paresthesia or paresthesia-like events may occur. Expulsion or migration of the implant have been reported, including rarely to the chest wall. In rare cases, implants have been found within the vasculature including the pulmonary artery. Some cases of implants found within the pulmonary artery reported chest pain and/or respiratory disorders (such as dyspnea, cough or hemoptysis); others have been reported as asymptomatic (see also Warnings under Precautions). Surgical intervention might be necessary when removing the implant.
On rare occasions, ectopic pregnancies have been reported (see Warnings under Precautions).
In women using (combined oral) contraceptives a number of (serious) undesirable effects have been reported. These include venous thromboembolic disorders, arterial thromboembolic disorders, hormone-dependent tumours (e.g. liver tumours, breast cancer) and chloasma, some of which are discussed in more detail in Precautions.
Note: The prescribing information of concomitant medications should be consulted to identify potential interactions.
Influence of other medicinal products on Implanon NXT: Interactions between hormonal contraceptives and other medicinal products may lead to breakthrough bleeding and/or contraceptive failure.
The following interactions have been reported in the literature (mainly with combined contraceptives but occasionally also with progestagen-only contraceptives).
Hepatic metabolism: Interactions can occur with medicinal or herbal products that induce microsomal enzymes, specifically cytochrome P450 enzymes (CYP), which can result in increased clearance, reducing plasma concentrations of sex hormones and may decrease the effectiveness of Implanon NXT. These products include phenytoin, barbiturates, primidone, bosentan, carbamazepine, rifampicin, and possibly also oxcarbazepine, topiramate, felbamate, griseofulvin, some HIV protease inhibitors (e.g. ritonavir) and non-nucleoside reverse transcriptase inhibitors (e.g. efavirenz), and the herbal remedy St. John's wort.
Enzyme induction can occur after a few days of treatment. Maximum enzyme induction is generally observed within a few weeks. After drug therapy is discontinued, enzyme induction can last for about 28 days.
When co-administered with hormonal contraceptives, many combinations of HIV protease inhibitors (e.g. nelfinavir) and non-nucleoside reverse transcriptase inhibitors (e.g. nevirapine), and/or combinations with HCV medicinal products (e.g. boceprevir, telaprevir), can increase or decrease plasma concentrations of progestins, including etonogestrel. The net effect of these changes may be clinically relevant in some cases.
Women receiving any of the previously mentioned hepatic enzyme-inducing drugs or herbal products should be advised that the efficacy of Implanon NXT may be reduced. If it is decided to continue using Implanon NXT, women should be advised to also use a non-hormonal contraceptive method during the time of concomitant drug administration and for 28 days after discontinuation.
Concomitant administration of strong (e.g. ketoconazole, itraconazole, clarithromycin) or moderate (e.g. fluconazole, diltiazem, erythromycin) CYP3A4 inhibitors may increase the serum concentrations of progestins, including etonogestrel.
Influence of Implanon NXT on other medicinal products: Hormonal contraceptives may interfere with the metabolism of other drugs. Accordingly, plasma and tissue concentrations may either increase (e.g., cyclosporin) or decrease (e.g., lamotrigine).
Laboratory parameters: Data obtained with combined OCs have shown that contraceptive steroids may affect some laboratory parameters, including biochemical parameters of liver, thyroid, adrenal and renal function, serum levels of (carrier) proteins, e.g., corticosteroid binding globulin and lipid/lipoprotein fractions, parameters of carbohydrate metabolism and parameters of coagulation and fibrinolysis. The changes generally remain within the normal range. To what extent this also applies to progestagen-only contraceptives is not known.
Magnetic Resonance Imaging (MRI) Safety Information: Implanon NXT is MR safe.
Incompatibilities: No incompatibilities are known.
Instructions for use and handling: See Dosage & Administration.
The applicator is for single use only.
Store below 30°C.
Shelf life: The shelf life of Implanon NXT is 5 years when stored as indicated.
G03AC08 - etonogestrel ; Belongs to the class of progestogens. Used as systemic contraceptives.
Implanon NXT implant 68 mg
1's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
